Question of the Week - November 2021
November 3rd, 2021

A 47-year-old female with a history of Aspirin-Exacerbated Respiratory Disease (AERD) presents to your clinic for an endoscopic sinonasal surgery evaluation. Patient was diagnosed with AERD last year, and has since been treated with multiple rounds of nasal sprays, antibiotics and low-dose systemic steroids with minimal relief. One of her CT scans is shown below:
When confirming the diagnosis of AERD, each of following could be taken into consideration EXCEPT:
A. Presence of nasal polyps on rigid endoscopy or CT scan
B. History of use of NSAIDs before the onset of asthma
C. 6-month-history of chronic rhinosinusitis
D. Watery eyes and wheezing after intranasal ketorolac
-
B (Understanding of AERD/Samter's Triad)
Samter's Triad includes the presence of bronchial asthma, nasal polyps, and aspirin intolerance. Intranasal ketorolac/oral aspirin is often used to establish the diagnosis of AERD. The history of the use of NSAIDs before the onset of asthma should not be taken into consideration, because patients develop hypersensitivity to NSAIDs AFTER the onset of asthma.
November 17th, 2021
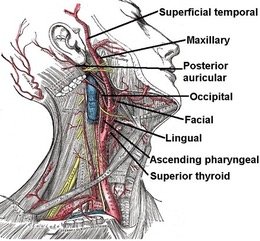
A 57-year-old female with a known history of atrial fibrillation taking eliquis is under a great deal of stress during a recent move to a new home. She has mistakenly packed up all of her medications and goes over a week without taking her anticoagulation. She presents to the ED with new symptoms of left facial deep muscle pain and weakness. On exam, she has an absent pulse in the area behind her left ear and her left temporal region. Her left face is not pale. Based on her symptoms, where is the anatomic defect?
A. At the common carotid
B. Internal carotid artery
C. Proximal to the facial artery
D. Proximal to the posterior auricular artery
E. At the terminal external carotid artery bifurcation